
{kind=link}
It’s been a long time since I’ve had a real alternative cancer cure testimonial to dissect that didn’t involve, for instance, ivermectin or fenbendazole, the new laetriles of the post-COVID era. So it was with interest that I was tagged on X, the hellsite formerly known as Twitter, and discovered FitScript™:
I had never heard of Michael Morelli before, nor had I heard of his service, Fitscript. After a flurry of questions and pushback, Mr. Morelli posted this:
To finish off the long post, so that you don’t actually have to visit X unless you want to, I’ll add the completion:
Healing of any kind only works when done on an individual basis specifically for the person.
Social media is full of generic advice that people think they should follow as it’s worked for someone else.
Our treatment for people is based on them as an individual and is unique to them. It’s what separates us from the others – so what we did for Paula is just an example of how effective we are.
It ALL starts with your OWN FiTScript.
Oh, goody. The treatment is “unique” to each individual, and, oh boy, the rest of the thread is full of red flags. I realize that some of you don’t like reading long X/Twitter/Xitter threads, but I think it’s worth it to see the depths of quackery being plumbed here; that is, before I explain why Paula’s testimonial does not demonstrate that anything Morelli did contributed to her being cancer-free:
David Grimes posted a good thread about why this is all nonsense. You can’t cure cancer with diet, and restrictive diets in particular are potentially harmful to cancer patients.
Although it’s been touted as a cancer cure since Linus Pauling in the 1970s, there remains no good evidence that high dose intravenous vitamin C has anything more than a marginal effect on any cancer. Certainly, there is no evidence that it can cure cancer.
Those of you who have read some of the previous discussions I’ve done of alternative cancer cure testimonials will probably realize that immediately had…questions. Of course, before I get to those questions, I do note that a fair number of people pointed out that you can’t tell if a breast cancer is gone using blood work. True, tumor markers are sometimes used to assess response to treatment in patients with metastatic disease, but for the most part they aren’t a thing in breast cancer. As for what the markers were, I will get back to the post where he bragged about the hundreds of markers that had been checked. In the meantime, let’s look at the questions that I had:
- How was the cancer diagnosed?
- How large was it? Were there involved lymph nodes? What stage was it at diagnosis?
- What subtype was it (e.g., infiltrating ductal vs. infiltrating lobular carcinoma)?
- What was its marker status with respect to hormone receptors—estrogen receptor (ER) and progesterone receptor (PR)—and HER2?
- Did Paula ever undergo surgery to resect the primary tumor?
Such are the questions that I have asked ever since I became interested in this topic and first wrote a general post on how to approach alternative medicine cancer cure testimonials back in 2009. Indeed, even before I examine whether the quackery used might even have “worked,” I like to look at the patient’s story and show why the anecdote doesn’t even provide evidence that the cancer “cure” or intervention had any effect on the progress of the cancer. So let’s start with that, and then I’ll discuss FitScript itself.
Paula’s story
Getting back to the story of this woman named Paula. As nearly always is the case with testimonials like hers, let’s just say that Morelli left out some…very important…information. Can you guess what it was? I must admit that, while I wasn’t surprised to learn this, I was somewhat surprised about one aspect of it. Here are two Instagram post found by others of the woman, Paula Macedo Hood, that tell the tale:
I’m not sure what she means by a “double lumpectomy,” unless she had two primary tumors, which is possible. I do, however, have to wonder whether she meant “double mastectomy.” Unfortunately, the followup post does not clarify, although it does tell me what I needed to know:
We still don’t know the answers to all the other questions that I had, but in reality, for purposes of this one woman, it doesn’t matter. We know she had her breast cancer resected. We know that the resection had negative margins, which means that the tumor had a rim of normal breast tissue surrounding it and that the tumor didn’t go up to any of the cut edges of the specimen, and we know that she had negative axillary lymph nodes. Resection with negative margins is the goal of every curative breast cancer surgery, and finding negative nodes is a good prognostic sign, as tumor in the axillary lymph nodes means that the primary tumor has not spread past the breast. Whatever operation she had, though, later photos on her Insta suggest that it was probably not bilateral mastectomies, as she doesn’t look as though she did and, even if she underwent bilateral mastectomy with immediate reconstruction, I doubt she’d be back to weight lifting so soon afterwards, as shown in her more recent photos:
It turns out that she had a bilateral lumpectomy, which implies that she had two tumors, one in each breast:
We might not know enough about the clinical features of her cancer (or cancers) to make a definitive recommendation with respect to treatment, but we do know that she had surgery to remove her primary tumor(s). I am also glad that Ms. Hood is doing well enough to be back into weight training and physical fitness. I will, however, admit that I had expected that she would have had her surgery at the beginning of her story, soon after her diagnosis. That is the usual form of these alternative cancer cure testimonials that I’ve seen over the years. Usually, the patient has surgery and then decides to forego adjuvant therapies, such as chemotherapy, endocrine therapy (e.g., tamoxifen), or radiation. Then, as I like to say, they attribute their survival to the woo that they chose after their surgery, not to the surgery itself. This is a general principle of many alternative cancer cure testimonials for cancers normally treated with surgery; Chris Wark’s testimonial about how his quackery cured his colon cancer comes to mind, which became the basis of his entire business.
Since I haven’t reviewed this in a while, I thought that now would be a good time to review in more details why in general these sorts of breast cancer testimonials tell us nothing about whether the quackery being touted works. The treatment of breast cancer is divided into two phases, locoregional control (treatment of the disease in the breast and and axillary lymph nodes) and systemic control (prevention of distant metastases). Surgery and radiation therapy are modalities used for local control; chemotherapy and hormonal therapy, for systemic control. Adjuvant therapy is one of these modalities administered after surgery. Adjuvant radiation therapy will improve local control and lower the rate of recurrence in the breast. Adjuvant chemotherapy and hormonal therapy will improve systemic control and decrease the rate of development of metastases, which are usually what kill patients. Such adjuvant therapies are what I like to call “icing on the cake” of surgery.
The reason breast cancer testimonials sound so convincing is that most lay people don’t know a lot about the disease, particularly that surgery alone “cures” many breast cancers. Early stage cancers are cured by surgery alone more often than not, and a significant minority of patients with even large tumors and multiple positive lymph nodes still have fairly decent chance of long term survival with surgery alone. I’ll start with a very common example. In the case of a lumpectomy, the local recurrence rate in the breast can be as high 30-40%. Radiation can reduce it to less than 5-8%. That means that women who forgo radiation are still more likely than not to avoid local recurrence in their breast, particularly if their tumor is small. In terms of distant metastases, which is what kills in the case of breast cancer and virtually all solid malignancies, chemotherapy and hormonal therapy decrease the risk of systemic recurrence and improve overall survival. The improvement can be small on an absolute basis in patients with early stage cancers but becomes more impressive with more advanced operable tumors. Because many breast cancer patients will do well with surgery alone, clinical trials with large numbers of patients are needed to find true treatment effects due to adjuvant systemic therapies in early stage breast cancers. Indeed, one of the hottest areas of cancer research is to determine molecular characteristics of tumors that will allow oncologists to differentiate women with low risk disease, who could forego chemotherapy safely, from those with high risk disease, who would be far more likely to benefit. As it is now, we give chemotherapy to the many in order to benefit the few simply because we do not know which specific women will benefit.
These facts help to explain breast cancer survivors who have undergone surgery but decided to forego chemotherapy and/or radiation therapy in favor of “alternative” medicine (Suzanne Somers, for instance). When such patients have a tumor with a good prognosis, where recurrence is uncommon or have a more advanced tumor but are lucky enough not to recur, they attribute their survival not to the primary surgery, but rather to whatever alternative therapy they have decided to take, even though it almost certainly had nothing to do with their survival. To them, it was the alternative medicine that “saved” them, not good old-fashioned surgery. In contrast, women who opt for alternative therapy and then recur obviously don’t provide good testimonials to sell alternative medicine, which is why you almost never hear about them. They’re bad for business.
Revisiting the topic today after so many years, there is a further wrinkle in understanding alternative cancer cure testimonials for breast cancer. The wrinkle doesn’t change the essence of the problem with these testimonials, namely that it’s the surgery and not the woo that cured the cancer, but things have changed—and fairly recently, as in during last few years—when it comes to the treatment of certain subtypes of breast cancer. For the most common type of cancers, the hormone receptor (ER/PR)-positive cancers with negative HER2, the old standard and order of treatments still generally apply: surgery, followed by radiation for breast-conserving surgery and then endocrine therapy to block estrogen with tamoxifen or a type of drug called an aromatase inhibitor . One reason that I asked for markers is that other subtypes of breast cancer at certain stages are now treated with neoadjuvant therapy (chemotherapy first), followed by surgery and then radiation, often with targeted therapy added in. For instance, if the tumor is positive for amplification of the HER2 oncogene regardless of hormone receptor status, then the treatment order is neoadjuvant chemotherapy plus HER2-targeted drugs, usually trastuzumab (Herceptin) and pertuzumab (Perjeta), followed by surgery and radiation. Based on the KEYNOTE-522 trial published in 2020, triple-negative cancers (negative for all three markers) that are greater than 2 cm in diameter are now treated with neoadjuvant chemoimmunotherapy consisting a combination of chemotherapy drugs plus an immunotherapy with pembrolizumab (Keytruda), followed by surgery. There are also studies of neoadjuvant endocrine therapy for hormone receptor-positive/HER2(-) tumors, but this is not standard of care for most such tumors; so that’s all I’ll say about it for now.
Both regimens, KEYNOTE-522 for triple-negative breast cancer and neoadjuvant chemotherapy plus HER2-targeting for HER2(+) cancers are so successful that they can produce pathologic complete response rate (pCR, no living tumor detectable in the surgical specimen after surgery) up to over 60%, to the point where there are now trials to determine whether surgery is even needed after a clinical complete response (the tumor is no longer detectable on physical exam or imaging), along with how to determine whether a clinical complete response is indeed a pCR. (When there isn’t a pCR, what is often found are microscopic nests of residual tumor cells.) None of these new advances in breast cancer treatment changes the overall problem with Paula’s alternative cancer cure testimonial, though, nspecifically that she had surgery.
In fact, thinking about this, it occurred to me that a smart quack (which Mr. Morelli does not appear to be) would tout his woo in a patient like Paula as “neoadjuvant” treatment before surgery, but he didn’t do that. Basically, he claimed that FitScript and the “treatments” guided by it did it all and didn’t even mention Paula’s surgery until after he was called out. Of course, one can’t help but note that, if his quackery actually did cure the cancer, then why did Paula decide three years after her diagnosis that she would undergo surgery? To me that suggests that, best case, the cancer wasn’t going away, or, worst case, that it had been getting bigger, leading Paula to decide to let a surgeon remove it and check her lymph nodes. Let me also say that it’s great that she had her tumor successfully removed and that her lymph nodes were negative. That’s what we try to achieve in the breast and want to see in the lymph nodes. That means that her prognosis is most likely good, although it would be better if she were to agree to the recommended adjuvant therapies, which would be guided by her cancer stage and tumor markers. I hope that she changes her mind.
I would also point out another thing. Let’s, for the sake of argument, accept that whatever “tumor markers” being followed by her functional medicine quack are actually science-based and reliable. (They’re almost certainly not—see next section—but let’s just assume for the moment that they are.) It seems not to occur to anyone that maybe—just maybe—the reason they are now zero is because she had her primary tumor surgically removed in January.
Hilariously, when called out by someone who had found Paula’s Instagram, Mr. Morelli basically blamed the functional medicine quack who had treated her and his social media team, while scoffing that he “doesn’t care what you think”:
You see? It’s faith-based. Mr. Morelli just knows that woo based on his test cured Paula. He just knows. Moreover:
Indeed, if you look at the FitScript website, you’ll find Mr. Morelli’s bio:
Years ago, I was far from the picture of success. Bankrupt, divorced, and struggling with addiction, my life was a far cry from where I stand today.
But I’m hardly an overnight success story. At the age of 31, I was a bankrupt and newly divorced drug addict living on my mother’s couch.
In and out of rehab for a decade, I’d built a $5 million business and lost it all. But hitting rock bottom was the start of something new.
Facing fatherhood, I took a hard look at my life. I knew it was time to make radical changes. In just 113 days, I went from 25% body fat to 8%, but it was more than just a physical transformation.
Hint: 8% body fat is the sort of level that competitive bodybuilders strive for. It’s very low and not necessarily healthy. Indeed, one thing that I’ve learned since I started resistance training is that even bodybuilders usually don’t try to stay at 8% all the time because it’s too difficult and not necessarily healthy. (In women, such a percentage body fat of 10-12% or lower will often shut down menstruation, for instance.) They get there when preparing to compete and then tend to go for 10-15% body fat the rest of the time. Let me just say that there’s nothing wrong with bouncing back after hitting bottom. Normally that would be quite admirable. What’s not so admirable is bouncing back by selling quackery like functional testing and functional medicine.
In response, Mr. Morelli basically bragged about his lack of qualifications:I
Not really. We’re just calling out grift and quackery from an unqualified entrepreneur when we perceive it. Again, there are no “results.” Paula’s anecdote doesn’t demonstrate that Mr. Morelli’s woo cured Paula. What it demonstrates is that she was fortunate enough to have a tumor that was growing slowly enough that she could wait three years to have it surgically resected and it (probably) didn’t spread to distant organs and become incurable.
But what about FitScript and the woo?
Functional medicine and FitsScript: Reams of useless tests revisited
I once described functional medicine as “reams of useless tests in one hand, a huge invoice in the other,” and FitScript appears to fit the bill perfectly. Let’s revisit the tests in the video posted to X on Saturday:
The narrator brags about 124 markers, 87 from blood, the rest from urine. The first thing that I noticed is that a lot of these are pretty standard labs with blood work, such as a complete blood count (CBC), which is broken down into its four individual components, which, I guess, count as four. Practically everyone gets a CBC whenever bloodwork is drawn, in order to detect anemia or abnormalities in white blood cell (WBC) or platelet counts. Of course, as functional medicine quacks often do, there are also a lot of thyroid function tests, whether indicated or not, plus a bunch of nonstandard tests. From this, apparently FitScript comes up with an estimated likelihood of dysfunction in various body systems ranging from blood sugar regulation to kidney function to thyroid function, which is questionable but not too far outside what regular doctors do. Of course, they can’t resist adding measures for “toxicity” or “toxic load,” because nearly all quacks blame nearly all health conditions on “toxins,” which seem so mystical, magical, unidentifiable, and amorphous that I sometimes like to refer to them as evil humors, which is what they resemble. The key here is that, based on massive overtesting, functional medicine doctors then try to “correct” every nutritional deficiency that they find by selling you supplements, whether the “deficiency” is real or clinically significant or not.
Indeed, there’s a reason why I describe functional medicine as the “worst of both worlds.” In a nutshell, functional medicine combines the massive overtesting to which conventional medicine can become prone with the quackery of alternative medicine in order to “correct” these tests. Moreover, if you order enough tests, by random chance alone some of them will be outside of the normal range. In an ideal world, where the “normal” range of a test is the 95% confidence interval around the mean found in a “normal” population, that would mean that roughly 5% of the lab values would likely be “abnormal” and need “correcting. Now look at this screenshot from the FitScript website:
Elsewhere on the website:
We analyze 124 biomarkers for health, the most comprehensive in the industry, covering everything from functional body systems to nutrient deficiencies.
Compare this to a standard blood test with just 12 to 20 biomarkers, and you’ll see why our approach is leaps and bounds ahead.
Because, apparently, more is always better. Not for quacks like Mr. Morelli and his team of functional medicine are standard panels of blood tests with a mere 12-20 biomarkers. He does 124 and apparently organizes them into 600 different biomarker combinations, thus increasing the chance for false positives. But customers love it:
Remember, one of the core “principles” of functional medicine is “biochemical individuality.” While it is true on a trivial level that no two people are exactly the same, that doesn’t mean that there is so much “individuality” that everyone will require a perfectly individualized plan or treatment for them. I’m also particularly amused by the claim that they can somehow tailor-make an exercise training program “as unique as your DNA.” If there’s one thing I’ve learned since I started going to the gym and engaging in resistance training, it’s that anyone who makes a claim that inflated is nearly always full of…well you know what. Training programs are, of course, personalized to the person, but not to the level of being “as unique as your DNA.” Another “tell” here is the “tailored supplement recommendations.” Basically, FitScript exists to sell you supplements to “correct” lab abnormalities and “nutritional deficiencies” that might or might not (probably not) need correcting, all according to plans cooked up by the company’s functional medicine quacks.
In any post about functional medicine, I feel compelled to remind our readers that the principle of each person’s “biochemical individuality” is, in essence, a “get out of jail free” card for basically anything its practitioners want to do. They can always find ways to justify any form of treatment, be it science-based or quackery, simply by invoking the “biochemical individuality” of the human being whom they are treating. I also like to remind my readers of my retort to this: Yes, human beings are individuals, and each human being is unique. However, we’re not so unique that our bodies don’t all work pretty much the same way. In other words, in terms of biology, physiology, and yes, systems biology, human beings are far more alike than they are different. If that weren’t the case, modern medicine, developed before we had the tools to probe our genetic individuality, wouldn’t work as well as it does. Functional medicine fetishizes “biochemical individuality”, not so much because humans are so incredibly different that each one absolutely has to have a markedly different treatment. We’re not. Functional medicine fetishizes “individuality” because it distinguishes functional medicine as a brand distinct from science-based medicine and, I suspect, because it makes functional medicine practitioners feel good, like “total” doctors never at a loss for an explanation for a patient’s symptoms or clinical condition, and makes patients feel like special snowflakes whose every bit of “individuality” is being catered to. In brief, functional uses science the same way a drunk uses a lamp post – not for illumination, but for support.
Speaking of quacks, the functional medicine practitioner in FitScript is Paul Burgess, who is described as “a trailblazing entrepreneur renowned as the visionary founder of two highly esteemed entities: Paul Burgess Functional Medicine Ltd, a global telehealth practice, and Paul Burgess Wellness, a transformative healthcare clinic.” I checked out his practice website and was amused to find how he described some of his treatments. For instance:
DNA testing for a truly bespoke exercise and nutrition plan, only you have your DNA so why follow a diet that everyone else does?
We are now able to unlock your genetic code and develop a diet and program specific to you and your goals.
All the guesswork is taken out so you can be sure that your time and effort is not wasted, either in the kitchen or in the gym.
Again, this is utter nonsense, and his use of the word “bespoke” to describe the exercise and nutrition plans that he comes up with are a huge tell. That’s not a word that we generally use in medicine, but rather in tailoring or other services in which a product is made for an individual customer.
The whole industry of DNA testing to come up with “individualized” nutrition and exercise plans is a topic too big to discuss here. Suffice to say, it’s the Wild West out there, with little that is truly evidence-based.
I did find something interesting on the website. Paula Hood is featured there as a success story:
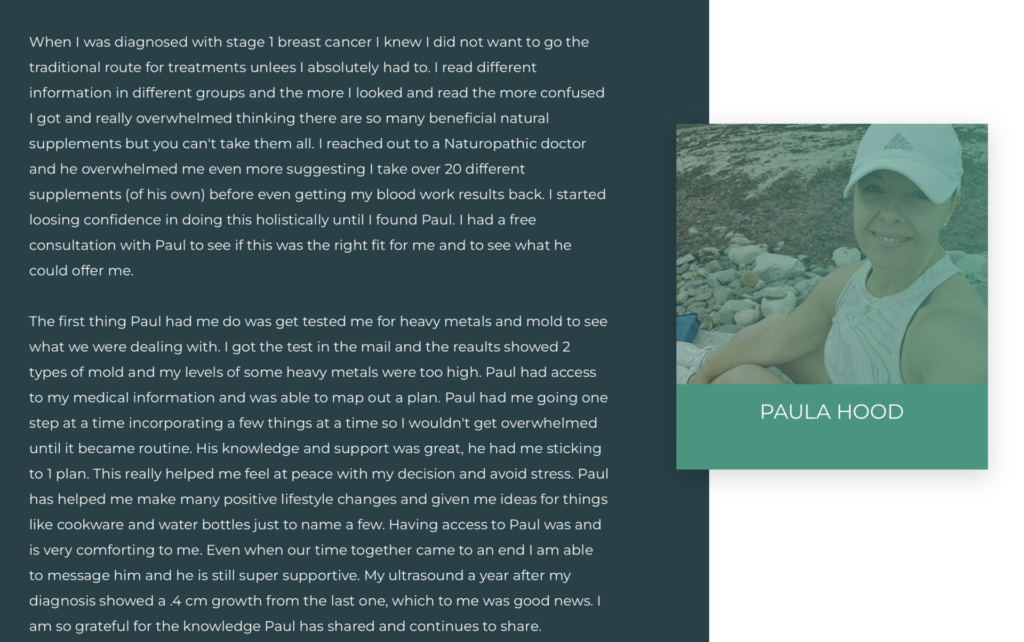
First, I called it. Her tumor had grown, and no doubt that is why she decided to undergo surgery. In other words, the quackery wasn’t working, and so a surgeon saved her. Also, this suggests that I was correct that her tumor was likely fairly slow growing and indolent, given that it had only grown 0.4 cm in the absence of treatment and she in essence waited three years to have any science-based treatment for it at all. Moreover, any tumor that’s been present for three years but hasn’t yet gone to the lymph nodes is not a particularly aggressive tumor. Basically, Ms. Hood is a great example of survivorship bias in that she gambled and, fortunately for her, won. I expect that she will likely do well no matter what she does, although absent at least radiation therapy she does have a pretty high risk of a recurrence in the breast. She’s fairly likely to get away with it, though, and I hope for her sake that she does.
Another thing is that I couldn’t find anywhere whether Paul Burgess is an actual doctor or not…of anything. He appears to be a health coach, which is all that his website seems to claim. I did find this elsewhere:
Paul Burgess has been a healthcare provider for over 20 years. Having had a keen interest in health from a very young age, Paul gained qualifications and began exploring different modalities. About 15-20 years ago, Paul decided to make revolutionising healthcare his main pursuit, finding it more fulfilling than anything else. Rather than having healthcare on the side as a “hobby”, where many practitioners struggle commercially and don’t get paid enough, Paul committed to developing his practice into a proper commercial business. He currently has a global online practice.
“Gained qualifications and began exploring different modalities”? What does that even mean? To me, it means that he’s not a physician and probably not even a naturopath. Otherwise, he’d trumpet that on his website.
So what we have with FitScript are two quack/entrepreneurs named Michael Morelli and Paul Burgess who epitomize my characterization of “functional medicine” as “reams of useless test results in one hand, a huge invoice in the other.” This would be bad enough if all they were doing was “treating” the worried well, but they’re not. They’re victimizing cancer patients like Paula Hood. I only hope that Ms. Hood ultimately realizes her mistake—as she realized her mistake of not undergoing surgery, although apparently without admitting that it was a mistake as her tumor grew while she was being treated with Morelli and Burgess’ quackery—and decides to undergo appropriate adjuvant treatment with radiation and whatever systemic therapy is recommended to minimize her chances of recurrence.
ADDENDUM 5/20/2024: A reader sent me a link to a Facebook post by Ms. Hood dated March 21, 2022. In the comments, she tells what her tumor markers were:
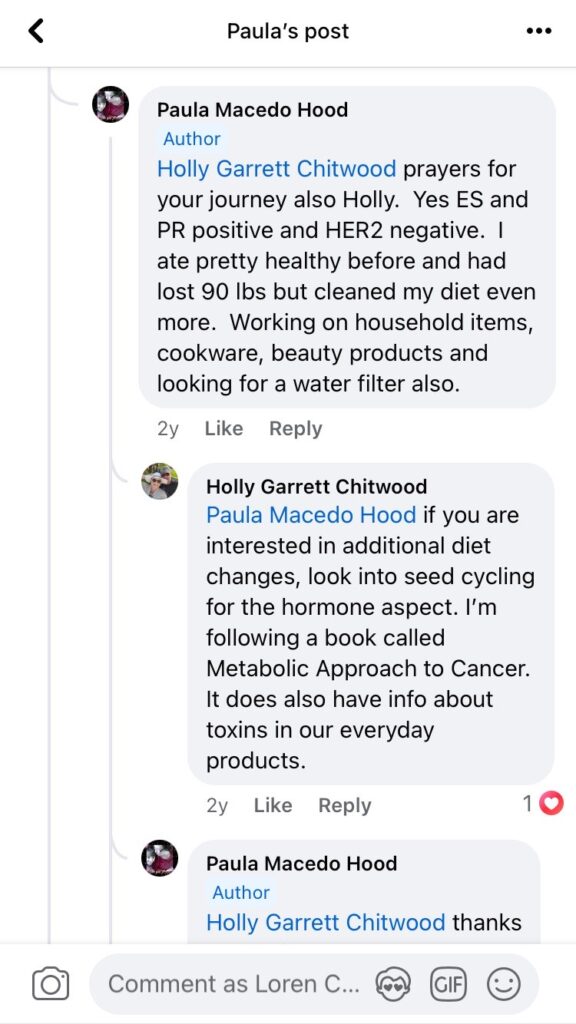
ER(+)/PR(+)/HER2(-) is the most common subtype of breast cancer; two-thirds of breast cancers have this marker combination. This type of tumor doesn’t need adjuvant chemotherapy, although if you want to get technical we do recommend chemotherapy if the tumor (1) has positive axillary lymph nodes and/or (2) has a high recurrence score on various gene-based tests like OncoType or Mammaprint, but that’s just getting into the weeds. The most important thing is that we do generally recommend endocrine (estrogen-blocking) therapy with tamoxifen (premenopausal women) or an aromatase inhibitor (postmenopausal women) for these tumors, and Ms. Hood apparently isn’t getting that. If she truly wants to maximize her chances of never having a recurrence and never dying of her breast cancer, I hope that Ms. Hood will accept radiation therapy followed by appropriate endocrine therapy, most likely tamoxifen given her age.